Understanding Male Pattern Baldness: Causes, Stages & Solutions
A clinical guide to androgenetic alopecia in men, covering the Norwood scale, genetic factors, and all available treatment options.
Male pattern baldness affects roughly half of all men by the age of 50 and nearly 80 percent by age 70. Despite those staggering numbers, most men who notice their hair thinning have very little understanding of why it is happening, how fast it will progress, or what they can actually do about it. This guide breaks down the clinical reality of androgenetic alopecia, from the molecular biology of DHT to the practical decision of choosing between medication and surgery.
What Is Androgenetic Alopecia?
Androgenetic alopecia is the medical term for the hereditary form of hair loss that follows a predictable pattern in men. The name itself provides a clue to its two driving forces: "androgen" refers to male hormones, and "genetic" points to the inherited sensitivity that determines whether those hormones will cause hair loss in any given individual.
Unlike other forms of hair loss that can strike suddenly or in random patches, androgenetic alopecia is gradual and patterned. It typically begins with a receding hairline at the temples and thinning at the crown, eventually merging to leave a horseshoe-shaped ring of hair around the sides and back of the head. This remaining hair persists because the follicles in those regions are genetically resistant to the hormonal signals that cause miniaturization elsewhere on the scalp.
The Role of DHT in Hair Loss
The primary hormonal culprit behind male pattern baldness is dihydrotestosterone, commonly known as DHT. DHT is produced when the enzyme 5-alpha reductase converts free testosterone into this more potent androgen. While DHT plays important roles during puberty, helping to develop male secondary sex characteristics like facial hair and a deeper voice, it has a destructive effect on genetically susceptible scalp follicles.
When DHT binds to androgen receptors on vulnerable hair follicles, it triggers a process called follicular miniaturization. Over successive growth cycles, the affected follicle produces thinner, shorter, and lighter hairs. A follicle that once generated a thick terminal hair may eventually produce only a fine, nearly invisible vellus hair before ceasing production altogether. The follicle itself does not die immediately; rather, it shrinks progressively. This is a critical distinction, because it means early intervention can potentially reverse or halt the miniaturization process before the follicle is permanently lost.
It is worth noting that men with male pattern baldness do not necessarily have higher testosterone or DHT levels than men with full heads of hair. The difference lies in follicular sensitivity. Two men with identical hormone levels can experience vastly different outcomes if one has inherited follicles that are highly sensitive to DHT and the other has not.
Genetic Factors and Inheritance
The genetics of male pattern baldness are more complex than the popular claim that hair loss comes from your mother's father. While the androgen receptor gene, located on the X chromosome and therefore inherited from your mother, is one of the strongest genetic predictors, it is far from the only gene involved. Research has identified more than 200 genetic loci that contribute to baldness risk, many of which are on autosomal chromosomes inherited from both parents.
In practical terms, this means that looking at both sides of your family tree gives a more complete picture. If your father, maternal grandfather, and paternal grandfather all experienced significant hair loss, your risk is considerably higher. If only one relative was affected, your chances of developing the same pattern are lower but certainly not zero. Identical twins provide the most compelling evidence for the genetic basis of this condition: they nearly always share the same pattern and progression of hair loss.
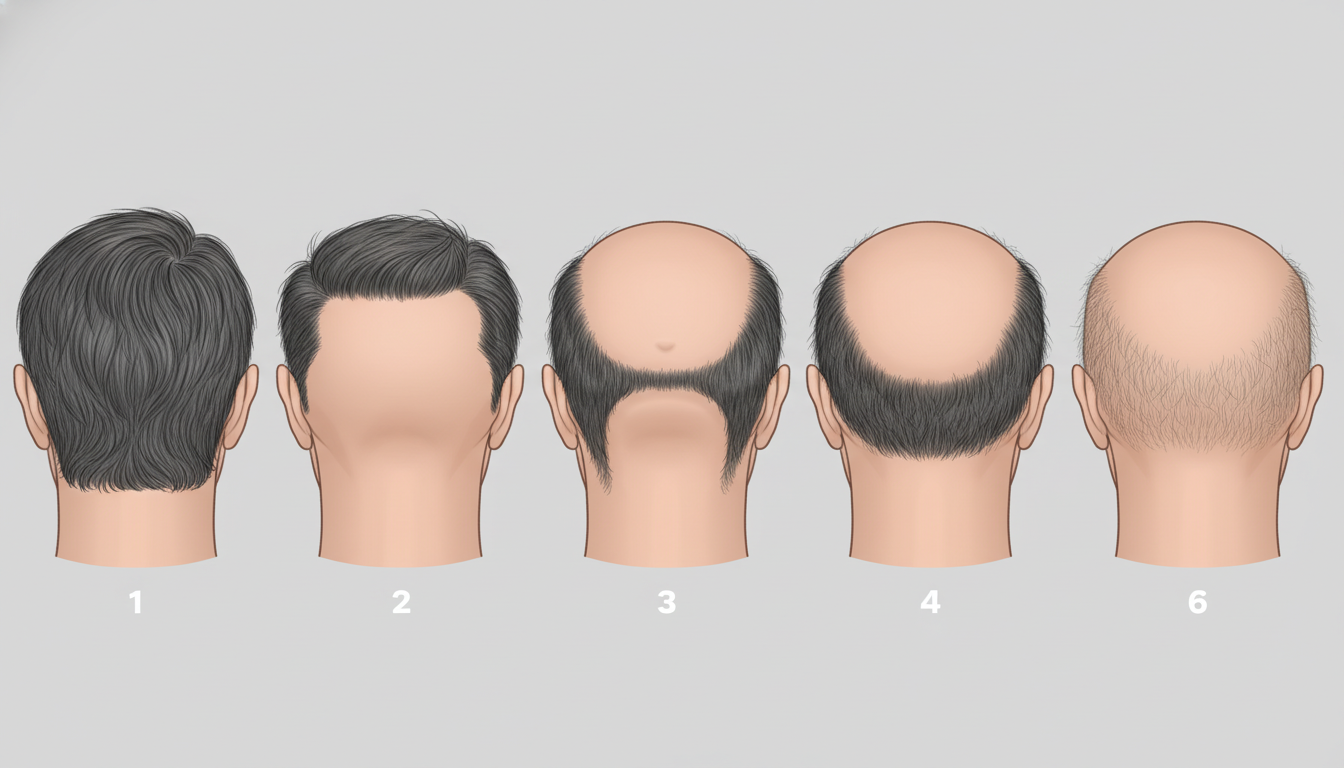
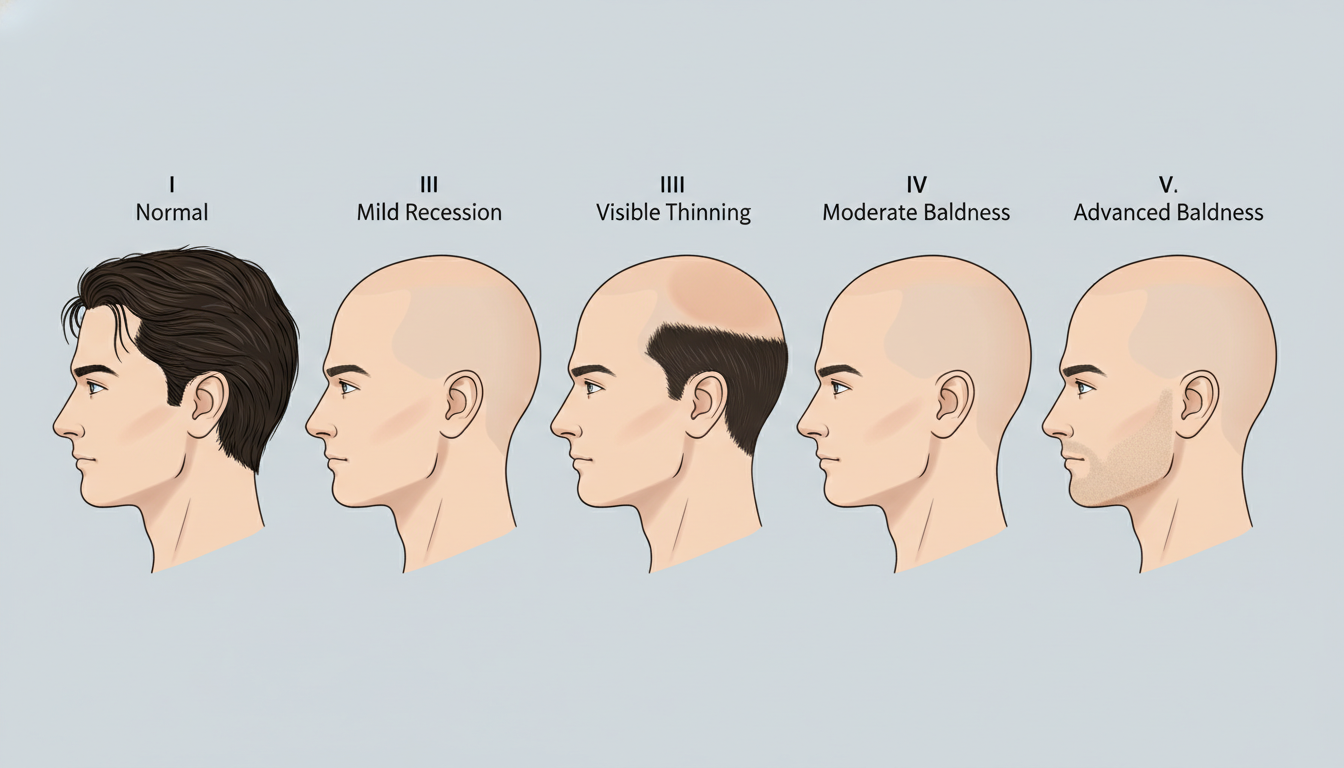
The Norwood-Hamilton Scale: Stages I Through VII
The Norwood-Hamilton classification system is the standard tool clinicians use to describe the extent of male pattern baldness. Understanding where you fall on this scale helps predict future progression and guides treatment decisions.
- Stage I: No significant hair loss or recession of the hairline. This is the baseline adolescent or pre-baldness hairline.
- Stage II: Slight recession at the temples, creating a more adult or mature hairline. Many clinicians consider this within normal range and not necessarily indicative of progressive loss.
- Stage III: The earliest stage considered clinically significant. Deepening temporal recession creates an M-shaped, U-shaped, or V-shaped hairline. Stage III Vertex is a variant with additional thinning at the crown.
- Stage IV: More severe recession at the front, combined with noticeable thinning or a bald spot at the crown. A bridge of moderately dense hair still separates the two areas.
- Stage V: The bridge of hair between the frontal and crown regions becomes thinner and narrower. The two zones of loss are beginning to merge.
- Stage VI: The bridge is gone. The frontal and crown bald areas have merged into one large zone, with only sparse hair remaining on top. The horseshoe pattern of remaining hair is clearly established.
- Stage VII: The most advanced stage. Only a narrow band of hair remains along the sides and back of the head. This remaining hair is typically thinner and may recede further over time.
Progression through these stages is not linear or predictable for every individual. Some men may advance rapidly from Stage III to Stage V within a few years, while others may remain at Stage III for decades. Age of onset is one of the most important prognostic factors: men who begin losing hair in their late teens or early twenties tend to progress more aggressively than those who start in their forties.
Early Warning Signs You Should Not Ignore
Detecting male pattern baldness early gives you the widest range of treatment options and the best chance of maintaining your existing hair. Watch for these signs:
- Increased hair on your pillow or in the shower drain. While losing 50 to 100 hairs per day is normal, a noticeable increase can signal the beginning of miniaturization.
- A widening part. If you part your hair in the same place and notice the part becoming visually wider, thinning may be underway.
- Scalp visibility. Being able to see your scalp through your hair in direct light, particularly at the crown, is a common early indicator.
- Temporal recession. Comparing current photos with those from a few years ago often reveals gradual recession that daily mirror checks miss.
- Changes in hair texture. Hairs becoming finer, softer, or lighter in color along the hairline or crown suggest follicular miniaturization is occurring.
Non-Surgical Treatment Options
Finasteride (Propecia)
Finasteride is an oral medication that inhibits the Type II 5-alpha reductase enzyme, reducing serum DHT levels by approximately 70 percent. For many men, this is enough to halt further hair loss, and a significant percentage experience some regrowth, particularly at the crown. Finasteride is most effective when started early, before extensive miniaturization has occurred. It requires ongoing daily use; discontinuation typically leads to resumed hair loss within 6 to 12 months. Side effects, which affect a small percentage of users, can include decreased libido and other sexual side effects. Discuss these risks thoroughly with your physician before starting treatment.
Minoxidil (Rogaine)
Minoxidil is a topical treatment available over the counter in 2% and 5% formulations. Originally developed as an oral blood pressure medication, minoxidil was found to promote hair growth as a side effect. Applied directly to the scalp twice daily, it works by prolonging the anagen (growth) phase of the hair cycle and increasing blood flow to miniaturizing follicles. Results vary, but many users see improved hair density after four to six months of consistent use. Like finasteride, the benefits disappear once treatment stops.
PRP Therapy
Platelet-rich plasma (PRP) therapy has emerged as a promising treatment for early-stage hair loss. The procedure involves drawing a small amount of the patient's own blood, processing it to concentrate the platelets and their growth factors, then injecting the concentrate into the scalp at areas of thinning. Research suggests PRP can stimulate dormant follicles and improve hair thickness. Many patients at our clinic combine PRP with other treatments for enhanced results.
Surgical Solutions for Hair Restoration
FUE Hair Transplant
Follicular Unit Extraction (FUE) is the most commonly performed hair transplant technique worldwide. The surgeon uses a tiny circular punch, typically 0.7 to 1.0 mm in diameter, to extract individual follicular units from the donor area at the back and sides of the head. These grafts are then carefully implanted into recipient sites created at the areas of thinning or baldness. FUE leaves no linear scar, heals quickly, and allows patients to wear their hair short without visible scarring. A single session can transplant anywhere from 1,500 to 4,000 or more grafts depending on the patient's needs and donor supply.
FUT Hair Transplant
Follicular Unit Transplantation (FUT), also known as the strip method, involves removing a narrow strip of tissue from the donor area, which is then dissected under microscopic magnification into individual follicular units. The donor site is closed with sutures or staples, leaving a thin linear scar that is easily concealed by surrounding hair. FUT can yield a higher number of grafts in a single session than FUE and may achieve a slightly higher graft survival rate because the follicles are not subjected to the mechanical stress of individual extraction. It remains an excellent option for patients who need maximum coverage and do not plan to shave their heads.
When Should You Seek Treatment?
The single most important principle in treating male pattern baldness is this: it is far easier to maintain existing hair than to regrow hair that has already been lost. Every month of delay allows more follicles to miniaturize, and some of those follicles will reach a point of no return where they can no longer produce visible hair even with treatment.
If you are in your twenties or thirties and noticing early signs of thinning, a consultation can help you understand your Norwood stage, assess the rate of progression, and build a treatment plan that may include medication, PRP therapy, or a future transplant strategy. Men in their forties and fifties who have more established hair loss often benefit from a surgical approach that can restore density to areas where medication alone cannot regenerate hair.
The patients who achieve the most natural and satisfying results are those who seek evaluation early. Even if you decide not to pursue immediate treatment, establishing a baseline allows us to track progression and intervene at the optimal time.
Combining Treatments for Optimal Results
Modern hair restoration is rarely about a single treatment in isolation. The most effective approach often combines multiple modalities. A patient might use finasteride to protect existing hair, undergo PRP therapy to revitalize miniaturizing follicles, and eventually pursue an FUE transplant to restore density in areas that medication cannot reach. This layered strategy addresses hair loss at multiple biological levels simultaneously.
For patients undergoing a hair transplant, continuing medical therapy post-operatively helps protect the native hair that was not transplanted. Without this protection, the non-transplanted hair may continue to thin, potentially creating an unnatural contrast between the transplanted and native zones over time.
Setting Realistic Expectations
Understanding what treatment can and cannot achieve is essential. No treatment can restore a Norwood VII patient to a full Norwood I head of hair. Donor supply is finite, and there are biological limits to what medication can regrow. However, skilled surgical technique combined with appropriate medical therapy can produce dramatic improvements that look completely natural and significantly improve quality of life.
The goal of hair restoration is not perfection but meaningful improvement. A well-designed hairline, improved density at the crown, and a sustainable long-term plan can give patients renewed confidence and a natural appearance that ages well over time.
Next Steps
If you are experiencing signs of male pattern baldness, the most productive first step is a professional evaluation. At Bellevue Hair Doctor, our board-certified specialists can assess your current Norwood stage, evaluate your donor area, discuss your goals, and recommend a personalized treatment plan. Whether you are a candidate for medical therapy, surgical restoration, or a combination approach, having accurate information empowers you to make the best decision for your situation.
Related Articles

Types of Alopecia Explained: From Androgenetic to Alopecia Areata
A comprehensive breakdown of alopecia types, how each progresses, and which conditions respond best to surgical vs. medical treatment.

FUE vs FUT: Which Hair Transplant Method Is Right for You?
A detailed comparison of Follicular Unit Extraction and Follicular Unit Transplantation covering scarring, recovery, cost, and graft yield.

PRP Therapy for Hair Restoration: What to Expect
How platelet-rich plasma therapy works, what a session involves, expected results, and how PRP complements hair transplant surgery.
Schedule Your Free Consultation
Have questions about hair loss or treatment options? Our board-certified specialists are here to help.